
 3405 8288
3405 8288Day Hernia Surgery
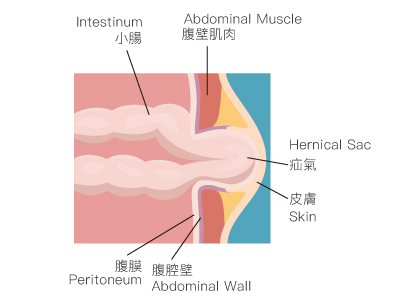
A hernia occurs when there is a defect in the abdominal wall, allowing internal tissues or organs, typically the intestines, along with the peritoneum, to protrude through a weak point in the abdominal cavity. This results in a noticeable bulge in the abdomen or groin.
Common Types of Hernias by Location:
-
Inguinal Hernia
-
Femoral Hernia
-
Umbilical Hernia
-
Incisional Hernia
Causes of Hernia
Under normal circumstances, the intestines are protected by the abdominal wall muscles. When the abdominal wall is weakened or the fascia is thin, increased pressure within the abdomen can cause the intestines to protrude through the defect, leading to a hernia. Generally, there are two primary causes of hernias:
- Congenital Factors: In children, a hernia may result from an incomplete closure of the processus vaginalis.
- Acquired Factors: In adults, hernias can develop due to a weakened abdominal wall, often associated with increased intra-abdominal pressure from chronic coughing, constipation, difficulty urinating, or heavy lifting.
Patients with hernias may observe a soft tissue bulge beneath the skin, particularly when standing, lifting heavy objects, laughing, coughing, or straining. This bulge generally disappears when lying down. Some patients may also experience mild discomfort, pain, or a dull ache.
Symptoms of Hernia
The symptoms of a hernia can be subtle. In mild cases, a soft tissue bulge may be visible during activities such as standing or coughing, typically occurring in the groin area, around the navel, or at previous surgical incision sites.
Common Symptoms Include:
- Bulge: The most prominent symptom is a noticeable bulge or swelling in the groin area, which is usually more evident when standing or coughing and may diminish when lying down.
- Discomfort or Pain: A hernia may cause discomfort or mild pain in the groin area, which can intensify with activity or prolonged standing, and may radiate to the scrotum or labia.
- Pressure Sensation: Patients may feel a sensation of pressure or burning, particularly after physical activity or prolonged standing.
- Increased Size with Coughing or Straining: The hernia bulge may enlarge or become more pronounced during actions such as coughing, sneezing, straining during bowel movements, or lifting heavy objects.
Are Men More Likely to Develop Hernias?
Individuals of any age can develop hernias; however, the incidence is significantly higher in men. Approximately 27% of men will experience a hernia compared to only 3% of women. Data from various hospitals indicate that over 400 cases of hernias are reported annually, with about 5% occurring in women, resulting in a male-to-female ratio of approximately 19:1.
Men are more susceptible to hernias due to differences in muscle tissue, pelvic structure, and abdominal fascia between genders. During embryonic development, the testes descend from the abdomen into the scrotum, passing through a canal that constricts after birth. If this canal does not close properly, it creates a weak point, allowing internal organs to protrude. In contrast, women typically have a narrower, shallower iliac fossa and a wider pelvic structure, reducing the likelihood of hernias.
Older adults are also at higher risk due to the degeneration of bodily tissues and functions, making them more susceptible to hernias.
Delayed Diagnosis and Treatment May Lead to Severe Complications
A hernia typically does not indicate a problem with the intestines themselves; however, when the intestine protrudes and becomes trapped at the hernia's edge, it can lead to serious complications such as intestinal obstruction or necrosis.
Due to the often subtle nature of hernia symptoms, many individuals may underestimate the potential severity of the condition. If a hernia is suspected, it is advisable for patients to seek prompt medical evaluation. Ignoring the condition may result in abdominal discomfort and, if the hernia enlarges and cannot be reduced, more serious complications may develop.
In severe cases, the trapped intestinal segment may become constricted, compromising its blood supply and leading to intestinal strangulation and necrosis, a life-threatening condition that necessitates emergency surgery to remove the affected segment of the intestine.
Patients experiencing symptoms or suspecting an abnormal protrusion in the abdomen should consult a physician for clinical evaluation. If clinical signs are not apparent, imaging studies such as ultrasound or computed tomography (CT) may be employed to assist in diagnosis.
Types of Hernias
Hernias are generally classified into four categories based on their location:
-
Inguinal Hernia: Occurs in the groin area.
-
Femoral Hernia: Occurs at the junction of the thigh and abdomen.
-
Umbilical Hernia: Occurs near the navel, leading to protrusion around the umbilicus.
-
Incisional Hernia: Occurs at the site of a previous surgical incision or scar.
Risk Factors for Hernia Development
Several factors contribute to the development of hernias, including:
-
Gender: Men are more likely to develop inguinal hernias due to anatomical changes during the descent of the testes into the scrotum, which creates a weaker structure in the groin area.
-
Age: Increasing age is a risk factor for inguinal hernias, as the strength and elasticity of bodily tissues decline over time.
-
Genetic Factors: There may be a hereditary predisposition to inguinal hernias, with a family history increasing an individual's risk.
-
Increased Strain: Repeated heavy lifting, vigorous physical activity, chronic coughing, or straining can elevate pressure in the groin area, increasing the likelihood of hernia formation.
-
Weak Abdominal Muscles: Conditions that weaken the abdominal wall, such as muscle tears or postoperative recovery, can raise the risk of developing an inguinal hernia.
-
Increased Intra-abdominal Pressure: Chronic constipation, obesity, and pregnancy can lead to increased intra-abdominal pressure, thereby heightening the risk of hernia development.
Treatment and Prevention
As medication is ineffective for treating hernias, surgical repair is the primary treatment method. While most hernias are not immediately serious, if the intestine becomes trapped, it can lead to pain and severe complications such as intestinal obstruction or necrosis, necessitating urgent surgical intervention.
Even in cases where underlying conditions may complicate surgical risks, surgical repair is essential to prevent complications such as incarceration or strangulation of the intestine. Over time, the defect may enlarge, increasing the likelihood of recurrence after surgery.
Modern hernia repairs typically involve the use of mesh to reinforce weak areas of the abdominal wall. Surgical options include open repair and minimally invasive repair. Open surgery may be performed under local anesthesia or monitored sedation, without the need for general anesthesia. Minimally invasive surgery is particularly beneficial for patients with bilateral hernias. Both surgical methods have their advantages and disadvantages, and patients should engage in thorough discussions with their healthcare providers to understand the associated risks before making a decision.
Surgical Approaches
To address the issues caused by hernias, surgical repair is necessary. Traditionally, open hernia repair involves making a 5 to 10 cm incision at the site of the hernia. This procedure can often be performed as an outpatient procedure.
Minimally Invasive Surgery: This refers to laparoscopic hernia repair, where the surgeon utilizes a small incision at the umbilicus along with two additional small punctures in the lower abdomen to complete the repair. This approach can also address bilateral inguinal hernias.
Minimally invasive techniques result in reduced surgical trauma and pain, with several small incisions. Compared to open surgery, the risk of postoperative infection is lower, and the smaller incisions typically lead to less pain, facilitating faster recovery for patients.
Note: Minimally invasive surgery requires general anesthesia. Patients with chronic conditions such as coronary heart disease or those who have undergone major abdominal surgeries should consult their physician prior to the procedure.
Inguinal Hernia
An inguinal hernia occurs in the abdomen near the groin area. It develops when fatty or intestinal tissues push through a weakness in the abdominal wall near the right or left inguinal canal, which is located at the base of the abdomen. This may present as a swelling or lump in the groin or as an enlarged scrotum (the pouch containing the testicles). The swelling may be accompanied by pain. Adult males over 40 are significantly more likely to develop direct inguinal hernias than females.
Preparation
-
Fasting Instructions: Patients are generally required to fast for 6 hours before surgery. This means no food intake for 6 hours prior to the procedure, although a small amount of plain water is allowed until 2 hours before the operation.
-
Preoperative Medications: Patients should take any prescribed medications as instructed.
-
Pregnancy Notification: Inform your physician if you are currently pregnant or suspect you might be. Do not eat for four hours before the operation.
-
Before the procedure, the physician will conduct a brief consultation and examination, explain the examination process and risks, and obtain a signed consent form for the operation. Patients should also remove dentures, jewelry, and metal items prior to surgery.
Wound Care
-
Dressing: After surgery, the wound will be covered with a sterile dressing, which should be kept intact and dry.
-
Stitches: Most wounds will be closed with absorbable sutures that dissolve on their own, eliminating the need for removal. If non-absorbable sutures are used, they must be removed at the designated follow-up appointment.
-
Showering: If the wound is covered with a waterproof dressing, patients may shower as usual the day after surgery. After showering, ensure that the waterproof dressing remains clean and dry.
Procedure
-
You will receive intravenous (IV) sedation and be placed under anesthesia.
-
The surgeon will begin by making a 1 cm incision at the lower edge of the patient's belly button to insert the laparoscope, which is connected to a video camera and light source.
-
Next, a space is created between the abdominal wall and peritoneum. The surgeon uses the camera to visualize the defect in the abdominal wall and the location of the hernia on a monitor. Two additional half-centimeter puncture holes will be made in the lower abdomen. A slender instrument is then inserted to repair the hernia defect, and a mesh patch is placed to reinforce the area.
-
The mesh will strengthen the defect in the abdominal wall and facilitate recovery.
Follow-up and Recovery
-
Avoid Strenuous Activity: After surgery, patients should avoid vigorous physical activities, especially repetitive bending, heavy lifting, or intense exercise, to prevent excessive pressure on the wound. Doctors typically recommend avoiding heavy lifting and intense exercise for 4 to 6 weeks.
-
Dietary Adjustments: After surgery, your physician may recommend dietary modifications to prevent constipation and straining during bowel movements. This may include increasing dietary fiber intake, drinking plenty of water, and avoiding constipating foods.
-
Gas Recurrence: The risk of small intestine gas recurrence varies based on the type of surgery. It is advisable for patients to consult their physician to choose an appropriate surgical treatment plan.
Prevention Tips
-
When engaging in weight lifting or resistance training, follow your trainer's guidance, progress gradually, and avoid excessive effort that increases abdominal pressure.
-
Consume plenty of fruits and vegetables and stay hydrated to maintain regular bowel movements.
-
Lift heavy objects carefully or avoid them altogether.
-
Maintain a healthy weight to prevent obesity.
-
If you have chronic cough, benign prostatic hyperplasia, or similar issues, seek medical attention and manage your symptoms promptly.
-
After surgery, the wound will be covered with a sterile dressing, which needs to be kept intact and dry.
-
Most wounds will be sutured with soft threads. The soft threads will slowly dissolve and absorb automatically, so there is no need to remove the stitches.
-
If sutures need to be removed, they must be done on a designated date.
-
If the wound has been covered with a waterproof dressing, you can bathe as usual the day after the operation. Please keep the waterproof dressing dry and clean after bathing.
Our centre offers both traditional open hernia repair and minimally invasive laparoscopic surgery. Both procedures can be performed at our outpatient surgical centre, allowing patients to be discharged on the same day without the need for hospitalization.
References
Kulah B, et al. Presentation and outcome of incarcerated external hernias in elderly patients. The American Journal of Surgery. 2001 Jul 1;182(1):18-23.
Fitzgibbons Jr RJ, Forse RA. Clinical practice. Groin hernias in adults. New England Journal of Medicine. 2015 Aug 6;372(8):756-63.
香港衛生署. 《常見醫療問題 - 疝氣》. Available at : https://www.dh.gov.hk/tc_chi/health_information/health_topics/health_topics_hernias.html
Shakil, A., et al. Inguinal Hernias: Diagnosis and management. American Family Physician, 102(8), 487–492.
Mayo Clinic. Inguinal hernia - Symptoms & causes. Available at : https://www.mayoclinic.org/diseases-conditions/inguinal-hernia/symptoms-causes/syc-20351547
American Society of Anesthesiologists. Hernia - Symptoms & types of hernia surgery. Made for This Moment. Available at : https://www.asahq.org/madeforthismoment/preparing-for-surgery/procedures/hernia-surgery/#:~:text=Seek%20immediate%20medical%20attention%20if,is%20suddenly%20larger%20than%20before